Module 6: The Need for Behavioral Change as a Motivator
Module Overview
Throughout this book, I have shown how goals lead to motivated behavior but also how they can create stress and the need to engage in a different type of motivated behavior called coping to deal with them. We also need to figure out what the costs of this behavior are and whether we have the resources to deal with them
Sometimes the demands that lead to stress arise from the crazy amount of pressure we put on ourselves to succeed. Where does this come from? It could come from our personality traits such as being highly conscientious (Module 7) or a high achievement or power need (Module 8). Or maybe we have realistic goals but are a procrastinator. Or do not know how to plan tasks. Maybe we do all that well but do not find effective ways to relieve stress and replenish our adaptation energy, such as exercising, walking the dog, hanging with friends, etc. Maybe we have poor coping mechanisms such that we smoke when stressed or resort to alcohol and/or drugs to escape life. These types of maladaptive behaviors may need to be changed and why I have chosen to add a module to this book on behavior modification, which is a definite form of motivated behavior. In fact, we will discuss the motivation to change in a bit.
I consider this an application of motivation but place it earlier in the book than the rest of the application chapters, which start in Module 9. I felt it went nicely with the topics in Part II. But notice I have already referenced Modules 7 and 8 which follow this one. So, though it can go here, additional content to come will explain some aspects of why we engage in the behavior that we do and why change may be needed. It also may explain why some people are better at making the change stick than others, called maintenance. Still, I am comfortable with the placement of this module in the book.
Content Links to: PSYCH 328: Self-Control at Washington State University which covers behavior modification. Be advised that this is a snapshot of the course and not the whole course.
The material is also derived from my textbook/OER, Principle of Behavior Analysis and Modification (2017). The full text can be accessed by clicking here.
Module Outline
- 6.1. Understanding Behavior
- 6.2. Overview of the Process of Change
- 6.3. A Willingness to Change
- 6.4. Defining the Behavior and Goal Setting
- 6.5. The ABCs of Behavior and Functional Assessment
- 6.6. Strategies to Bring about Motivated Change
- 6.7. Implementing the Plan
- 6.8. Evaluating the Plan’s Success
- 6.9. Maintenance Phase and Relapse Prevention
Module Learning Outcomes
- Define and describe the characteristics of behavior.
- Clarify how the field of applied behavior analysis goes about changing behavior and describe the ABCs of behavior.
- Describe self-regulation and self-control and state their importance for behavioral change.
- Clarify stages people go through when deciding to bring about behavior change.
- Clarify the role of self-efficacy in behavior change.
- Clarify what a behavioral definition is and why it is important to applied behavior analysts.
- State the importance of setting clear goals in terms of what behavior you want to change.
- Describe the who, what, when, where, and why of recording and data collection.
- Clarify what is learned through a functional assessment and describe how to conduct one.
- Clarify the importance of the baseline phase.
- Identify strategies to help bring about change.
- Discuss the importance of the treatment phase in a behavior modification plan.
- Discuss why you need to evaluate and adjust your plan.
- State the importance of the maintenance phase.
- Explain the concept of relapse.
6.1. Understanding Behavior
Section Learning Objectives
- Define and exemplify behavior.
- List and define the four dimensions of behavior.
- Differentiate overt and covert behavior.
- Describe how behavior impacts the environment.
- Contrast basic and applied science.
- Describe the ABCs of behavior.
- Define self-management or self-modification.
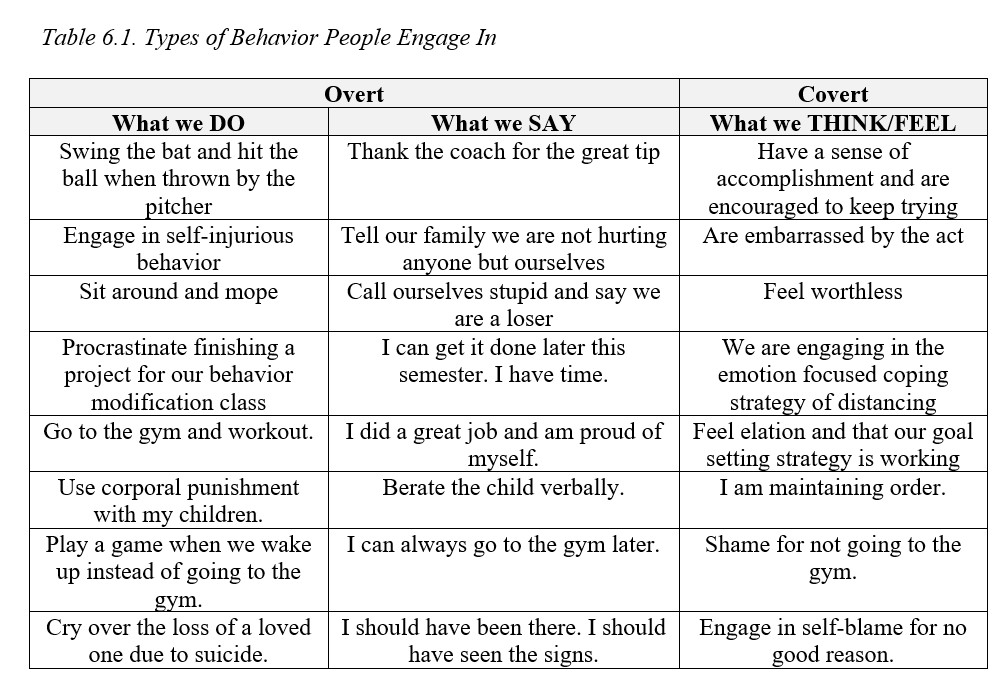
The focus of psychology is the scientific study of behavior and what causes it (mental or cognitive processes), while the focus of applied behavior analysis or behavior modification is changing behavior. Behavior is what people do, say, or think/feel. See Table 6.1 for examples. Behavior has several dimensions that are important to mention. They include:
- Frequency – This is how often the behavior occurs.
- Duration – This is how long the behavior lasts.
- Intensity – This is how strongly the behavior occurs.
- Latency – This is the time from when a stimulus presents itself and a behavior follows.
For any behavior we engage in, some number of these dimensions are important. For instance, if we see ourselves as worthless, often a sign of depression, we need to figure out how long the feelings have gone on for and how intense they have become. If the thoughts (and related symptoms) occur for a short duration but are intense, this is characteristic of Major Depressive Disorder. If they last a long time (long duration) but are not very intense, this is characteristic of dysthymia or mild depression. What about running? We need to know how often we run each week, how long we run, and at what speed – the dimensions of frequency, duration, and intensity respectively. Finally, consider a father asking his son to take the trash out as I often do with my son. If it takes him 15 minutes to do so, then this is the latency.
Behavior can be overt or covet. Overt is behavior that is observable while covert behavior cannot be observed. We might even call covert behavior private events. When a behavior is observable, it can be described, recorded, and measured.
Behavior also impacts the environment or serves a function. If we go into the bathroom and turn on the water, we are then able to brush our teeth. If we scream at our daughter for walking into the street without looking, we could create fear in her or raise her awareness of proper street crossing procedure. In either situation, we have impacted the environment, either physically, as in the example of the faucet, or socially as with the street incident. Here’s one more example you might relate to – your professor enters the classroom and says, “Put away your books for a pop quiz.”
Science has two forms – basic or pure/applied. Basic science is concerned with the acquisition of knowledge for the sake of the knowledge and nothing else; applied science desires to find solutions to real-world problems. You might think of it like this – the researcher decides on his own question to investigate in pure science, but an outside source often identifies the research question/problem in applied science. Of course, this is not always the case. In terms of the study of learning, the pure/basic science approach is covered under the experimental analysis of behavior, while the applied science approach is represented by applied behavior analysis (ABA).
So, what is applied behavior analysis all about? Simply, we must first undergo an analysis of the behavior in question to understand a few key pieces of information. We call these the ABCs of behavior, and they include:
- Antecedents – These are the environmental events or stimuli that trigger a behavior. If your significant other does something nice for you and you say, ‘thank you,’ the kind act is the antecedent.
- Behaviors – Again, this is what the person does, says, thinks/feels. In the previous example, you saying, ‘Thank you,’ is the behavior or what you said. The behavior may be something we want to increase, and so is classified as a behavioral deficit, or something we need to decrease and is a behavioral excess. As we will discuss later, we will have desirable and undesirable behaviors we engage in. The undesirable serves as temptations and distract us from our end goal.
- Consequence – You might say a consequence is the outcome of a behavior that either encourages it to be made again in the future or discourages its future occurrence. If we always engage in a particular behavior when a specific stimulus is present, then there must be some favorable outcome that follows the behavior, thereby reinforcing its occurrence and making it highly likely that the behavior will occur the next time the antecedent is present. Hence why we say that the antecedent is a trigger for the behavior.
Behavior modification can be used to change the behavior of others but note that the same principles and procedures can be implemented by an individual to bring about their own change. This is called self-management or self-modification.
6.2. Overview of the Process of Change
Section Learning Objectives
- Differentiate self-regulation and self-control.
- Outline the process of change and its steps.
6.2.1. Self-control
Before we dive into the process of change, I wanted to briefly comment on the fact that to make a change we must have discipline. In some cases, we adjust our behavior based on the feedback we receive from others. Joking around with our significant other after he or she had a long and hard day at work will be perceived differently than a day in which he/she received an exemplary performance evaluation and a raise. Or the feedback may come from ourselves, such that we stop working out because we notice our heart rate has reached dangerous levels or we turn off the television because we are distracted. Our ability to carefully consider our actions and the effect they have on others or ourselves, and to make such adjustments, is called self-regulation. We self-regulate or self-direct more than just our actions. We can also control our thoughts, feelings, attitudes, and impulses. You might think of self-regulation as a form of behavior modification but in the short term. It could be long term too. To lose weight, we have to exercise on a regular basis, watch what we eat, drink water, manage our stress, and get enough sleep. A few days of doing this will not produce the results we seek. We need to stay committed for many months or even years.
This leads to the topic of self-control and avoiding temptations. It takes a great deal of discipline to not sleep in, get fast food for dinner, stay up late watching Netflix, or let demands in our environment overwhelm us. This is sometimes called brute self-control (Cervone, Mor, Orom, Shadel, & Scott, 2011) and if it goes on for too long can leave us in a weakened state and cause giving in to our desires (McGonigal, 2011).
Note that Skinner (1953) did not see self-control as willpower, the term that is commonly used, but more so involving outcomes or the consequences of engaging in a behavior. If we eat ice cream after a hard day and it makes us feel better (NR — taking away an aversive feeling or say the frustration from the day) we will be more likely to eat ice cream again as comfort food. If we are on a diet, this can wreak havoc. Though we may feel better in the short-term, we will feel guilty in the long-term when faced with weight gain. He discussed things we do to alter how often a response occurs. The altered response itself is called the controlled response and the responses that do the altering are called controlling responses. If we decide to watch a funny movie to feel better after a hard day instead of eating ice cream, then the movie is a controlling response, and the ice cream is the controlled response. We might also use something discussed in a bit called self-instructions and talk ourselves through a better way to deal with the stress of the day (also a controlling response).
6.2.2. Steps in the Process of Change
The process of change involves the following steps. Be advised that these are not universal but my conceptualization of the order, though most other textbook authors use similar steps. Some parts of the process must occur in a specific order. For instance, you cannot implement your plan without first having an idea of what strategies you would use. You cannot do that without having an idea of the ABCs of the behavior. And to start the whole process off you must know what behavior you want to change, by identifying the target behavior. A plan concludes with a maintenance phase, and you have to know when to go to it by evaluating your success. So again, there can be some variability with some steps and their order, such as determining the plan to record and establishing goals. They generally occur about the same time and 5 could go before 4.
Figure 6.1. Steps in the Process of Change
Planning for Change
- 1. Identify the Target Behavior
- 2. Conduct a Pros and Cons Analysis and Assess Self-Efficacy
- 3. State the behavioral definition
- 4. Establish goals and criterion
- 5. Determine a plan to record data
- 6. Conduct a baseline phase and functional assessment, to include an identification of temptations
- 7. Select strategies
- 8. State the plan rules, identify potential mistakes, and develop a behavioral contract
Implementation and Behavior Change
- 9. Implement the plan and collect data as you go – Treatment phase
- 10. Re-evaluate the plan and see if it is working. Make adjustments as needed
11. Once you have achieved your final goal move to maintenance phase. Engage in relapse prevention
6.3. A Willingness to Change
Section Learning Objectives
- Outline the steps of change according to Prochaska et al. (1995).
- Define self-efficacy.
- Contrast those high and low in self-efficacy.
- Clarify how self-efficacy affects the success of a behavior modification plan
6.3.1. Thinking About Changing
Prochaska, Norcross, and DiClemente (1995), in their book, Changing for Good, state that “Change is unavoidable, part of life. Few changes are under our control. But some things we can intentionally change.” How so? We must initiate change to help modify thoughts, feelings, or behaviors. They also say, “In change, timing is everything” and nine processes are involved. A few of interest are countering in which we substitute healthy responses for unhealthy ones, helping relationships or asking for help from your loved ones so you don’t have to go it alone, rewards or giving yourself a special prize when you achieve your goal and minimizing the use of punishment, commitment or accepting responsibility for the change on a personal level and then “announcing to others your firm commitment to change,” and conscious awareness or bringing unconscious motivations to a conscious level.
Knowing when to change is key because if you are not ready, you will inevitably fail. Likewise, if you spend too much time trying to understand your problem you might put off change indefinitely. Change unfolds through a series of six stages and successful self-changers follow the same road for each problem they desire to modify. These stages include: precontemplation, contemplation, preparation, action, maintenance, and termination. Let’s look closely at each.
6.3.1.1. Precontemplation stage. This is when the person is not considering making a change and even resists the idea. Control of the problem is shifted to outside the person and they do not want to be nagged about the problem from family and friends. The individual even denies responsibility for the problem and justifies the behavior.
Prochaska, Norcross, and DiClemente (1995) suggest the individual answer the following questions to help them see the difference between problem behaviors and lifestyle choices:
- Do you discuss your behavior pattern?
- Are you well informed about your behavior?
- Are you willing to take responsibility for the consequence of your behavior?
Individuals move out of the precontemplative stage when they realize that their environment no longer supports their unhealthy lifestyle, when there is social pressure to make the change, or they receive direct requests from others such as employers.
6.3.1.2. Contemplation stage. This is when change is seriously considered, but within the next six months. Many people stay stuck in this stage for a long period of time due to a fear of failure and so postpone and procrastinate. We have made the decision to change, but when the time is right. Of course, we all know there is no such time. We also engage in wishful thinking and desire to live as we always have but with different consequences such as eating what we want and not gaining any additional weight.
The authors state that you know you are ready to move on when your focus is on the solution and not the problem. We need to engage in consciousness-raising by asking the right questions such as understanding how many calories we really need to consume each day or what the effects of smoking are on the body and how long it will take to recover from them, if we can at all. We might also set goals, collect data, and do a functional assessment. In any case, it is critical to engage in this task during the contemplation stage as it helps us to be more aware of our problem behavior, “gain insight into how your thinking and feeling maintain the problem, and begin to develop a personal conviction of the value of change” (Prochaska, Norcross, and DiClemente, 1995).
You can even engage in a process of self-reevaluation, which if successful, will show that your fundamental values conflict with the problem behavior. We might assess how unhappy we are with the habit or behavior in the present, and then engage in an appraisal of our happier, healthier changed selves in the future. We could also think before we act especially with problems involving overeating, smoking, or drinking; create a new image of a changed you; and evaluate the pros and cons of changing.
6.3.1.3. Preparation stage. This is when the person gets ready to change within the next month. Make your intention to change public and develop a firm, detailed plan for action. In terms of the plan, be specific about what steps you will take to solve the problem. Commitment involves a willingness to act and a “belief/faith in your ability to change.” Engage in social support also at this time, even if you decide not to make your plan for change public.
6.3.1.4. Action stage. Now fully committed to change, we enter the action stage. This requires a great deal of time, energy, and sacrifice. We must be aware that the action stage is “not the first or last stop in the cycle of change.” The action stage lasts for months and involves being aware of potential pitfalls we may encounter.
It is during this stage we engage in the process of change called countering, or substituting a problem behavior with a healthy behavior. Of course, all we may do is substitute one problem behavior for another, but to minimize that possibility, we could engage in active diversion by keeping busy or refocusing energy into an enjoyable, healthy, and incompatible activity. We might exercise, relax, counterthink by replacing troubling thoughts with more positive ones, or be assertive, especially if others in your life are triggering the problem behavior. Though resisting temptation is an accomplishment, it is not rewarding enough, and so we need to be rewarded when we counter, exercise, relax, counterthink, or be assertive. Helping relationships are also important to make our success more likely.
6.3.1.5. Maintenance stage. This is when change continues after the first goals have been achieved. To be successful, your change must last more than just a few days or months. It should last a lifetime. To be successful at maintenance Prochaska, Norcross, and DiClemente (1995) state that you should have long-term effort and a revised lifestyle. Relapse is a possibility if you are not strongly committed to your change.
How do you maintain your positive gains? Stay away from situations or environments that are tempting. Our former problems will still be attractive to us, especially in the case of addictive behaviors. What threatens us most are “social pressures, internal challenges, and special situations.” In terms of internal challenges, the authors state that these include overconfidence, daily temptation, and self-blame. Creating a new lifestyle is key too. If we are under a great deal of stress, exercise or practicing relaxation techniques instead of engaging in our former behavior of comfort eating or drinking alcohol.
6.3.1.6. Termination stage. This is when the ultimate goal has been achieved but relapse is still possible. Actually, Prochaska, Norcross, and DiClemente (1995) note that, “Recycle is probably a more accurate and compassionate term than relapse. Recycling gives us opportunities to learn.” How so? They note that people pass through the stages not in a linear fashion but more in a spiral. It may seem like we are not making progress, but the spiral is ever pushing upward. Also, few changers ever terminate the first time around unless they have professional help or a clear understanding of the process of change.
See also: McConnaughy, DiClemente, Prochaska, and Velicer (1989) and Prochaska and DiClemente (1992)
6.3.2. Self-Efficacy
Change is not easy and the more of a change we have to make, the more difficult or stressful. This is where Albert Bandura’s concept of self-efficacy (Bandura, 1982, 1986, 1991a, 199b) comes in. Self-efficacy is our sense of self-esteem and competence and feeling like we can deal with life’s problems. It includes our beliefs about our ability to complete a task and affects how we think, feel, and what motivate ourselves. When our self-efficacy is high, we feel like we can cope with life events and overcome obstacles. Difficult tasks are seen as challenges, and we set challenging goals. In contrast, if it is low, we feel hopeless, helpless, and that we cannot handle what life throws at us. We avoid difficult tasks and throw in the towel quickly when things get tough. These individuals are easily depressed and stressed.
Consider this in relation to how successful we might be with achieving our goal of changing an unwanted behavior or establishing a positive behavior. The pros and cons of changing the behavior (Note: I skipped this for the purposes of this book) if weighing heavier on the side of making a change, give us the motivation or desire to make a change. But having the desire does not mean that change will occur. We need the ability and, possibly more important, we have to believe we can make the change. The change itself is the obstacle to overcome and is challenging for us. If it was not, we would have made the change already. Those high in self-efficacy will be more likely to move from the action stage to maintenance and termination of the treatment plan compared to those low in self-efficacy.
An example will hopefully help you to understand the relationship between willingness and ability. In terms of losing weight, many people genuinely desire to shed unwanted pounds. They engaged in a pros and cons analysis and the pros won out. But many do not understand how to lose weight in terms of making sense of caloric intake, the impact of specific foods they eat, consumption of sugars and protein, the role of sleep and water intake, etc. Armed with this knowledge they can be successful. Their ability would match their desire to make a change. But many do not know these important facts and so lose some weight early on but then stagnate and give up. Losing the pounds is motivational or reinforces the weight reduction behaviors being used, leading to a continued commitment to the plan (a type of NR). But when weight loss stagnates, we become frustrated and return to the behaviors that caused the problem in the first place.
6.4. Defining the Behavior
Section Learning Objectives
- Define and exemplify behavioral definition
- Clarify how a criterion is used to move from one goal to the next.
6.4.1. Behavioral Definitions
It is critical to clearly define what the behavior is you wish to change. In behavioral modification, we call this a behavioral definition. A behavioral definition is a precise, objective, unambiguous description of the target behavior or a competing behavior. Our behavior may be an excess and something we need to decrease, or a deficit and something we need to increase. No matter what type of behavior we need to change, we must state it with enough precision that anyone can read our behavioral definition and be able to accurately measure the behavior when it occurs. Let’s say you want to exercise more. You could define it as follows:
- 1 behavior = going to the gym and using a cardio machine (elliptical, treadmill, or stationary bike) for 20 minutes.
Okay, so if you went to the gym and worked out for 40 minutes, you would have made 2 behaviors. If you went to the gym for 60 minutes, you made 3 behaviors. What if you went to the gym for 30 minutes? Then you made 1.5 behaviors, correct? No. It does not make sense to count behaviors by the half.
Behavioral definitions should be simple. Do not make it reflect whatever your end goal will be. For instance, if your overall goal is to run for 60 minutes, do not make your behavioral definition to be 1 behavior = 60 minutes of running. Since we do not count partial behaviors, you will show no behaviors made until you finally reach 60 minutes of running. How low should you go then? If 60 is too high, do you define it as 1 behavior = 1 minute of running? Likely not. Think about what is the least amount of time you would run. If it is 5 minutes, you could set it at 1 behavior = 5 minutes of running. Then if you run 30 minutes you would have made 6 behaviors. With defining running as 20 minutes of continuous exercise you can only count 1 behavior and the other 10 minutes are unaccounted for. Think about what denomination of time is most practical for your situation and where you are starting out at. If you have never run before, a smaller increment of time might be better. If you run about 30 minutes a few days per week and want to simply double your time, then you could use a greater increment such as 10, 15, or 20 minutes.
We should always create behavioral definitions for the target behavior but also any competing behaviors that may occur. If we want to go to the gym more often, we might discover when examining our antecedents that playing games on our phone in the morning or talking to our roommate in the afternoon leaves us with not enough time to work out. We would then define this competing behavior, or a behavior that interferes with the successful completion of a target behavior, and then when developing our plan, implement strategies that make the distractor less, well, distracting.
6.4.2. Goal Setting
Once you have an idea of exactly what the behavior is you want to change, the next task is to set goals about the behavior. This involves the same information we discussed in Module 3: Goal Motivation. In behavior modification, you have your distal goal and to get there, use proximal or subgoals.
But how do we know when to advance from one goal to the next. The specific “trigger” for when to advance from Goal 1 to Goal 2 is called the criterion. Our first goal states that we will run for 15 minutes 3 days a week. Achieved. When do we move to running 30 minutes for 3 days a week? That depends on the behavior we are trying to change. In exercise related projects or plans, it is prudent to make sure you can truly engage in that level of behavior for at least two weeks. Listen to your body, a trainer or doctor, and then move to the next goal when it is safe to do so. For other projects such as pleasure reading, you could move to the next goal as soon as the current goal has been achieved. There is no need to wait as no serious harm can come from increasing the number of pages you read a night from 5 to 10, other than a few minutes of lost sleep.
6.5. Determining the ABCs of Behavior via a Functional Assessment
Section Learning Objectives
- Define self-monitoring.
- Clarify what the observation period is.
- Differentiate between a natural setting and an analogue setting.
- Clarify the use of the ABC chart in data collection.
- Describe the importance of the baseline phase.
- Define functional assessment.
- Outline what information is gained from a functional assessment.
- Define temptation.
- Explain how people and things can be temptations.
- Clarify the significance of situations and places and how they might lead you to engage in the undesired behavior.
- Propose ways to avoid giving in to temptations.
6.5.1. Collecting Data
6.5.1.1. Who does the recording? In terms of who does the measuring, this may be a professional or other individual routinely associated with the individual such as a teacher, work supervisor, counselor, school bus driver, caregiver, or sibling. In the case of self-management or self-modification, you are doing the measuring and recording which is called self-monitoring. One issue in behavior modification is what we call reactivity, or when the process of recording a behavior causes the behavior to change, even before treatment is applied. This may make obtaining baseline data to compare with treatment data difficult. If the nutritionist wants to reduce the consumption of high fat, salty foods in her client’s diet to help with weight loss she will need to know what the client eats normally. If the client alters his behavior upon knowing what the focus of the nutritionist is, then comparison data will not be possible. Of course, in the case of self-monitoring, the actual monitoring itself is part of the treatment and so we expect that keeping a food journal or using an app such as Fitbit will alter one’s behavior.
6.5.1.2. When do we record? In terms of when we record, we will have a clearly defined observation period and should choose a time when the behavior is likely to occur.
6.5.1.3. Where do we record? In terms of where, we can choose a natural setting or place where the behavior typically occurs, or an analogue setting or one that is not part of the person’s daily routine. This is the equivalent to naturalistic and laboratory observation, respectively. Finally, we can choose structured or unstructured events to observe which refers to whether or not there is a specific event or activity to observe and record.
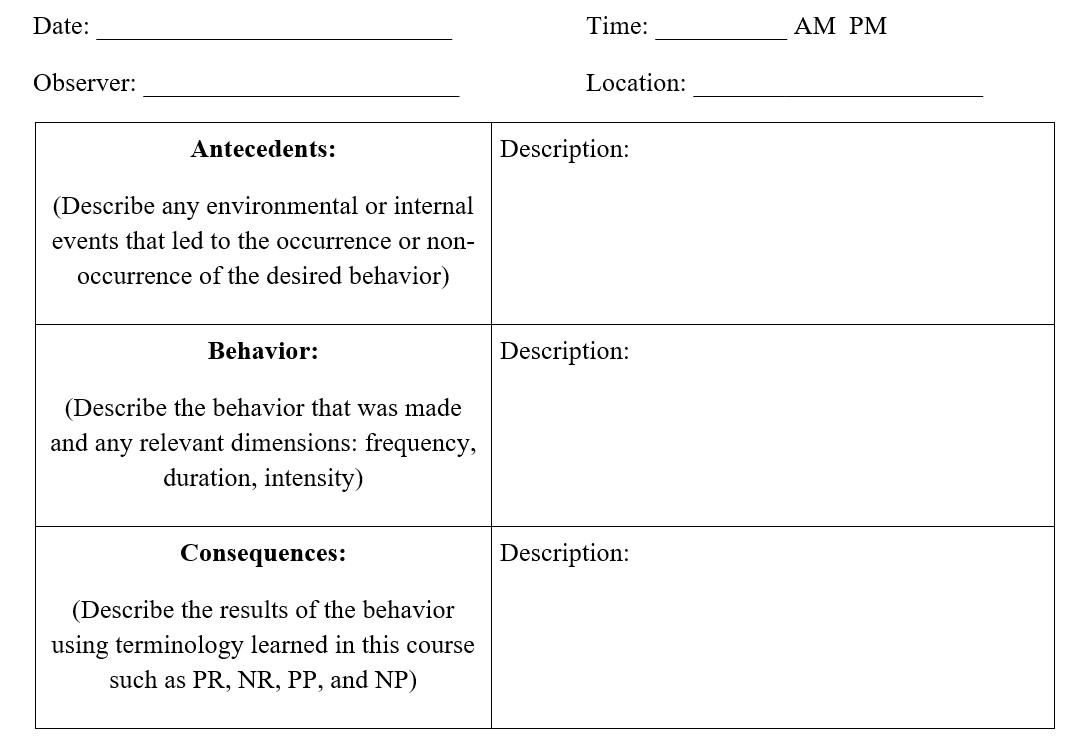
6.5.1.4. With what do we record? Recording can be done in many ways. You might record instances of the behavior using low tech options such as paper and pencil, moving coins from the left pocket to the right pocket, or tearing a sheet of paper. Alternatively, you can go high tech with a computer, phone, using barcodes, or tablets. Middle of the road alternatives include a pedometer, stopwatch, or golf stroke counter. No matter which method you use, you will ultimately want to record on what are called ABC charts (also called structured diaries). These tools record what environmental or internal events led to the occurrence of the behavior or the antecedent, what form the behavior took, and what happened afterward or the consequences. ABC charts can look like the following:
Figure 6.2. ABC Chart
6.5.2. The Baseline Phase
The baseline phase is when we collect data but do not attempt to change our behavior. No strategies are in place. We are trying to find out how often, long, or intensely we engage in our target/desirable behavior or a problem behavior. In cases when we are not making the desirable behavior at all, such as going to the gym or using a planner to organize our school work, a baseline phase is still useful for determining why we do not engage in the desired behavior and/or why we make a problem behavior. Typically, we continue with the baseline phase until a clear pattern emerges and this can take a few days at least.
After your behavior modification plan has run its course, you will compare the level of your behavior after the strategies were used against the level of the behavior before they were used. As such, the baseline phase serves as a comparison with the treatment phase.
6.5.3. What is Functional Assessment
A functional assessment is when we much more closely scrutinize the antecedents and consequences to see what affects the occurrence or nonoccurrence of a desired or problem behavior, all to maximize how effective our plan/strategies will be. This data comes from an analysis of what we recorded on our ABC charts during the baseline phase. This scrutiny involves gathering several important types of information about the behavior, antecedents, consequences, and previous interventions.
6.5.3.1. The behavior. What makes up the problem behavior or the desired behavior. It may be that in the case of a problem behavior, several sub-behaviors are included. For instance, earlier we described a student being disruptive in class. This is fairly general and could include the sub-behaviors of getting out of his seat without permission, talking without being called on, verbally or physically harassing other students, being uncooperative, ignoring directions from the teacher, or acting aggressively on the playground or during gym. These behaviors would be recorded on a baseline ABC chart.
6.5.3.2. The antecedents. What stimuli in the environment, or thoughts/feelings in the person, lead to the behavior’s occurrence/non-occurrence. These stimuli will actually predict the behavior in the future. To develop an effective plan, you must know what cues there are for the behavior but also make sure you go back far enough in time to find the true cue. If a person does not socialize, it could be due to worry about embarrassing him or herself but examining deeper reveals a parent who told the individual he was worthless and no one would ever like him. This reason would obviously need more work undoing/correcting than simply worry about looking foolish. Either way, it is safe to say or is predictable, that the individual will not strike up a conversation with another student waiting in line to pay for his textbooks early in the semester if there is concern about being embarrassed or subconsciously, you hear your parent’s voice and condescension. You will also want to know if there are certain situations, events, times, etc. that lead to the desired behavior or problem behavior.
6.5.3.3. The consequences. These are any events that follow the problem or desired behavior and maintain it. Face it. If you do not derive some benefit from making the behavior, there is simply no reason to make it. This goes for problem or desirable behaviors. If you wake up in the morning, play games on your phone, and really enjoy it, you will not be as concerned about getting to the gym to workout. The consequences are particularly reinforcing for you and maintain the problem behavior. If during the process of deciding to engage in behavioral change you decide that being in shape and losing weight is more important, you will encounter stronger reinforcers for working out then you do for playing games on your phone. You might even realize that while you are on the recumbent bike, you can spend a few minutes on your favorite game, so you are not losing out on this fun activity while you get in shape. In short, motivation is key and centers on consequences. You can look at your baseline phase ABC charts for indicators of motivators to engage in the desired or problem behavior or if anything negative occurred which led you to avoid the target behavior.
6.5.3.4. Previous interventions. It may be this is not your first time attempting to change the behavior. Maybe years ago, you changed it, maintained that success for several years, but then relapsed for any number of reasons. You will want your current applied behavior analyst to know what was part of your treatment plan before. Some elements may have worked while others may not have…then. Times change and so do people and you might find that video games were reinforcing 10 years ago but not so much today. Analyzing these interventions will help you to figure out what might work again, all while acknowledging a new approach may be needed. This information is not present in the baseline phase ABC charts but embedded in the client’s (or your) personal history.
6.5.4. Temptations – What You’d Rather Be Doing
Temptations are anything or anyone that might lead you to engage in the undesired or problem behavior and not make the desired or target behavior. What forms do temptations take? First, they can be a person such as a friend, who instead of encouraging you to watch your calories, asks you to go on late night Taco Bell run with them a couple times a week. Though you can always refuse to get food, you feel awkward being the only one not eating and make a purchase too. A thing can be an item that reminds you to engage in the problem behavior such as seeing the candy bars in the pantry or on the kitchen counter. The presence of the object (i.e. the candy) tempts you to pick it up and eat it, violating your weight loss plan. Situations are the conditions during which a temptation is likely to occur while places are the physical locations where temptations most likely will be present. An example of a situation might be sitting around and watching your favorite reality television show. When you do, you tend to pull out the popcorn, chips, ice cream, etc. In terms of places, let’s say you always eat fatty foods such as hot dogs, hamburgers, chips, candy, etc. and drink soda when you go to see your favorite football team play. You only do this when you are at the stadium and not when home watching the game. If you eat fatty foods while watching football in any location, then it is no longer a place but a situation.
Let’s try another example – drinking soda – using all four types of temptations:
- Person – Your best friend always has soda with him throughout the day and offers you one. It does not matter where he is or what time of day it is.
- Thing – You want a soda because you see an ad on television or in a magazine you like. It might also be seeing the Freestyle machine at your local restaurant. Or maybe you see a totally random person drinking a Cherry Pepsi and now you want one.
- Situation – You drink soda when you go to the movies because you like to have it with your popcorn. You also drink soda at home when you watch a movie and eat popcorn. Soda drinking is linked to watching movies specifically.
- Places – You only drink soda when you go to your town’s local movie theater. You love movie theater popcorn and need the soda to combat the saltiness of the popcorn, and the fact that you drown the poor popcorn pieces in the bucket in an ocean of butter (P.S. If you are concurrently running a weight loss behavior modification plan, STAY AWAY from the movie theater or at least the butter machine. Thank you. Now back to our regularly scheduled example). Or maybe you hate popcorn but love getting a soda at the movies because they have the Freestyle machine, and you love the seemingly endless options you have at a push of a button. No other establishment in your town has such a machine and so you purchasing a soda is linked to this one location/place.
6.5.4.1. What to do about temptations. Eventually you will give in to temptation if you need to exert self-control long enough. You only have so much and if you must constantly use it, you will run out. So even the “best” among us succumb to temptation at some point. The trick is to figure out ways to delay or manage this as much as possible. How so?
The simplest solution is to ask your friends not to tempt you. Let your friends know about your behavior modification plan and that you need their support. Make them stakeholders in your success so that they do not tempt you, or at least as much, and offer encouragement when you do a good job. But if you do give in, don’t blame them completely. You ultimately have the right to say no. Also, self-instructions are a great way to keep your goal in mind…or to keep your eye on the prize. In the moments when you are tempted, use positive affirmations or other statements about making the desired behavior.
You should also take note of anything you said to yourself when you gave in to the temptation. If you said something like, “just this one time,” then you might find yourself using the same logic on subsequent occasions when you are tempted. Realizing that you have done this in the past, and may do this again in the future, can help you to avoid the pitfall when it occurs.
Of course, the best advice that I can give is to not go to places where you know you will be tempted or enter into situations that you know always lead you to the problem behavior. It is sort of like obtaining a STD – you cannot get one if you practice abstinence. If you have to be in the situation, make it less tempting. If you are trying to lose weight and eating out late at night with friends is undermining your plan, then go out with friends but drink a protein drink before you leave so you are not hungry when you are there. Also, get water to keep your stomach mostly full.
6.6. Strategies to Bring about Motivated Change
Section Learning Objectives
- Define discriminative stimuli.
- Clarify how stimuli or antecedents become cues.
- List and describe the six antecedent manipulations.
- Define prompts.
- List, describe, and exemplify the four types.
- Define fading.
- List and describe the two major types of fading and any subtypes.
- Clarify the use of self-instructions in behavior modification.
- Clarify the use of social support in behavior modification.
- Describe how shaping can be used to modify a behavior.
- Describe strategies used to modify fear and anxiety behaviors.
- Describe strategies used to modify habit behaviors.
- Describe strategies used to modify maladaptive cognitions.
- Clarify how to use differential reinforcement in a treatment plan.
- Describe and exemplify the use of the token economy in a treatment plan.
- List, describe, and exemplify punishment procedures.
6.6.1. Overview
To start, recall that antecedents are the stimuli that lead to our behavior. We have seen this presented as S –> R –> C or A –> B –> C. The frameworks are the same. S and A are stimuli and antecedents and refer to environmental or internal causes of our behavior. R and B are the behavior(s) we are making and can include both the desirable behavior and any problem behavior(s). C is the consequence(s) of our behavior. When coming up with a treatment plan, you will likely use at least one strategy for each of the three components. Antecedents are especially important because if you have all the right triggers or cues in place, you are more likely to make the desired behavior and avoid making undesirable ones.
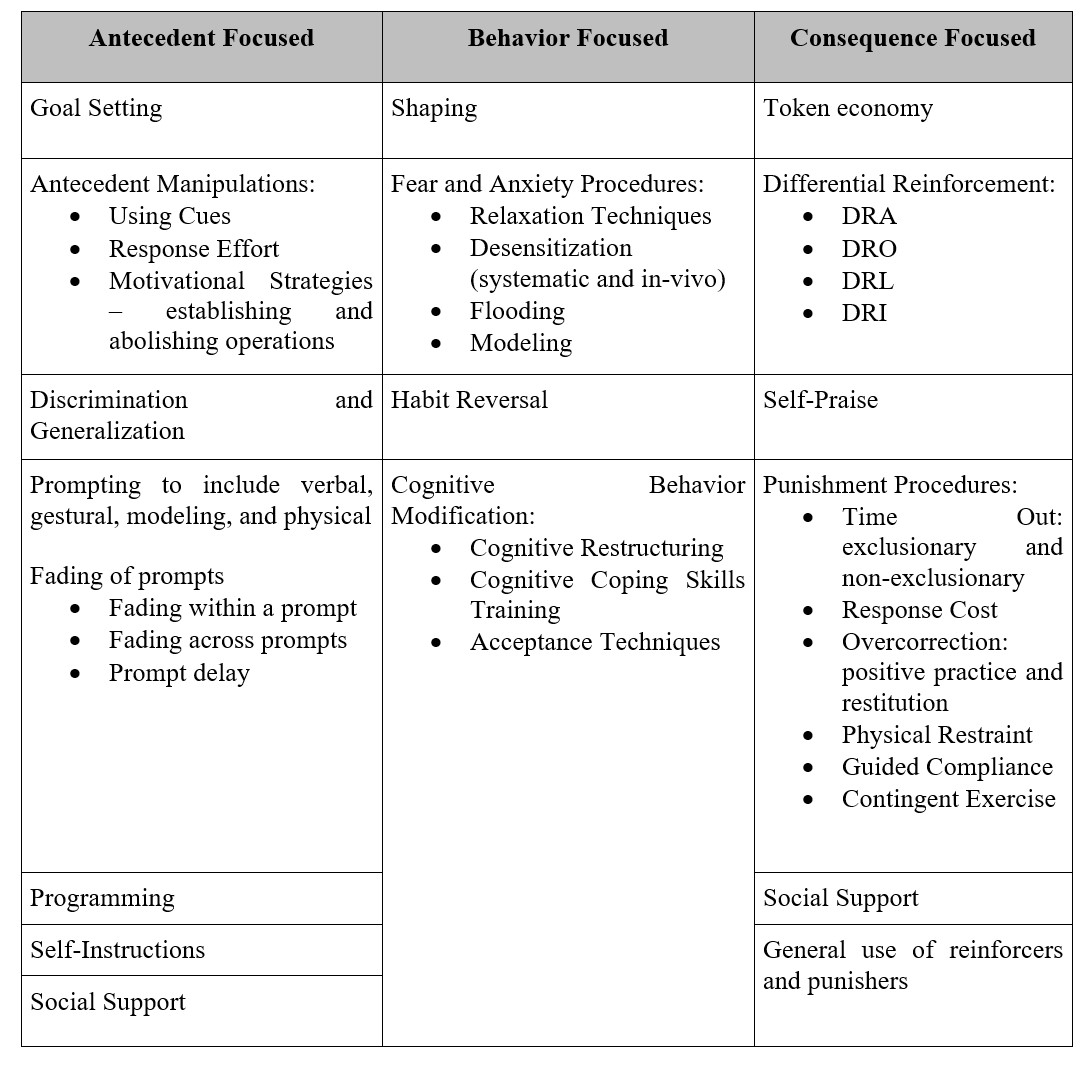
Table 6.2. Summary of Behavior Modification Strategies
6.6.2. Antecedent Focused Strategies
6.6.2.1. Antecedent manipulations. One critical step is to exert control over the cues for the behavior and when these cues bring about a specific behavior, we call them discriminative stimuli (also called a SD). So, what makes an antecedent a cue for a behavior? Simply, the behavior is reinforced in the presence of the specific stimulus and not reinforced when the stimulus or antecedent is not present.
The strategies we will discuss center on two ideas: we can modify an existing antecedent or create a new one. With some abusive behaviors centered on alcohol, drugs, nicotine, or food, the best policy is to never even be tempted by the substance. If you do not smoke the first cigarette, eat the first donut, take the first drink, etc. you do not have to worry about making additional problem behaviors. It appears that abstinence is truly the best policy.
But what if this is not possible or necessary? The following strategies could be attempted:
- Create a Cue for the Desirable Behavior – If we want to wake up in the morning to go to the gym, leave your gym clothes out and by the bed. You will see them when you wake up and be more likely to go to the gym. If you are trying to drink more water, take a refillable bottle with you to classes. Hiking around campus all day can be tough and so having your water bottle will help you to stay hydrated.
- Remove a Cue for the Undesirable or Problem Behavior – In this case, we are modifying an existing antecedent/cue. Let’s say you wake up in the morning, like I do, and get on your phone to check your favorite game. You initially only intend to spend a few minutes doing so but an hour later you have done all the leveling up, resource collecting, candy swiping, structure building, etc. that you can and now, you have taken your time to do a work out. In this case, the phone use is a problem behavior because it interferes or competes with the execution of the desirable behavior of going to the gym. What do you do? There is a simple solution – don’t leave your phone by your bed. If it is not in the room, it cannot be a reminder for you to engage in the problem behavior. The phone usage in the morning already exists as a behavior and the phone serves as a cue for playing games. You enjoy playing the games and so it is reinforcing. If the phone is not present then the behavior of playing the game cannot be reinforced and the cue loses its effectiveness. In the case of water, if we do not carry tea with us we cannot drink it, but can only drink our water bottle, thereby meeting our goal.
- Increasing the Energy Needed to Make a Problem Behavior – Since the problem behavior already exists and has been reinforced in the past, making its future occurrence likely in the presence of the stimulus, the best bet is to make it really hard to make this unwanted behavior. Back to the gym example. We already know that our phone is what distracts us and so we remove the stimuli. One thing we could do is place the phone in the nightstand. Out of sight. Out of mind, right? Maybe. Maybe not. Since we know the phone is in the nightstand, we could still pull it out in the morning. If that occurs, our strategy to remove the cue for phone usage fails. We can still remove it, but instead of placing it in the nightstand, place it in the living room and inside our school bag. So now it is out of sight, out of mind, but also far away which will require much more physical energy to go get than if it was in the nightstand beside us. Think about this for a minute. The strategy literally means that we expend more energy to do the bad behavior, than…
- Decreasing the Energy Needed to Engage in the Desirable Behavior – …we would for the good behavior. Having our clothes by our bed is both a cue to go to the gym, but also, by having them all arranged in one place, we don’t have to spend the extra time and energy running around our bedroom looking for clothes. We might also place our gym bag and keys by the door which saves us energy early in the morning when we are rushing out to the gym. What about for drinking water? Instead of carrying a water bottle with us we could just drink water from the water fountains at school. Okay. But let’s say that you are standing in the hallway and the nearest water fountain is all the way up the hallway and near the door to exit the building. You can walk up the hall, bend over, push the button, drink the water, remove your hand from the fountain, walk back down the hall, re-enter the classroom, and then take your seat. Not too bad, right? WRONG. If you had your water bottle in your backpack, you would only need to reach down, pick it up, open the bottle, take a drink, cap the bottle, and set it back down on the floor or on the desk. You never have to leave your seat which means you are making far fewer behaviors in the overall behavior of drinking water, and so expending much less energy. Now you can use this energy for other purposes such as taking notes in class and raising your hand to ask a question.
Another way you can look at antecedents is to focus on the consequences. We might focus on the motivating properties of the consequence so that in the future, we want to make the behavior when the same antecedent is present. Notice the emphasis on want. Remember, you are enhancing the motivating properties. How do we do this?
- First, we could use what are called establishing operations or when we enhance the reinforcing value of the consequence of a desirable behavior so that the same behavior occurs in the future when the same antecedent is present. Weight loss is really tough for most especially when there are so many yummy temptations out there. One solution is to find a cookbook or at least recipes that you really, really like. This will create excitement when dinner time comes and make it more likely that you stay on your diet…and want to. You have enhanced the reinforcing value of eating healthy and so in the future when your significant other says “What’s for dinner?” you can pull out your handy dandy recipe book/box/internet site and cook up something wonderful…and healthy. How about grocery shopping? If you want to eat healthy, don’t go to the store hungry or in a state of food deprivation. If you do, you are creating an establishing operation, but this time for the undesirable behavior. Think about that. If you can enhance the reinforcing value of a desirable behavior you can do so for an undesirable one too. Be careful.
- Second, we could use an abolishing operation and reduce the reinforcing value of an undesirable behavior. In the case of buying healthy foods, junk food is less desirable if we go to the grocery store full, or in a state of satiety. Do you really want to avoid eating pizza late night? Look up the nutritional information most every restaurant has available on their website or onsite. It is alarming just how calorie dense and fattening some of our favorites are. Ignorance is not bliss in this case. If you are on a weight loss program, recording your calories via an app like Fitbit or MyFitnessPal is not only a smart strategy, but necessary. Weight loss occurs when we take in less calories then we expend. Knowledge is power…and the power to make better choices.
6.6.2.2. Prompting and fading. Another great strategy that can be used is what is called prompts, or a stimulus that is added to the situation and increases the likelihood that the desirable response will be made when it is needed. The response is then reinforced. There are four main types of prompts:
- Verbal – Telling the person what to do
- Gestural – Making gestures with your body to indicate the correct action the person should engage in
- Modeling – Demonstrating for the person what to do
- Physical – Guiding the person through physical contact to make the correct response
These are all useful and it is a safe bet to say that you have experienced all of them at some point. How so? Let’s say you just started a job at McDonald’s. You were hired to work the cash register and take orders. On your first day you are assigned a trainer and she walks you through what you need to do. She might give you verbal instructions as to what needs to be done and when, and how, to work the cash register. As you are taking your first order on your own, you cannot remember which menu the Big Mac meal fell under. She might point in the right area which would be making a gesture. Your trainer might even demonstrate the first few orders before you take over so that you can model or imitate her later. And finally, if you are having problems, she could take your hand and touch the Big Mac meal key, though this may be a bit aversive for most and likely improper. The point is that the trainer could use all these prompts to help you learn how to take orders from customers. Consider that the prompts are in a sort of order from the easiest or least aversive (verbal) to the hardest or most aversive (physical). This will be important in a bit.
It is also prudent to reinforce the person when they engage in the correct behavior. If you told the person what to do, and they do it correctly, offer praise right away. The same goes for them complying with your gesture, imitating you correctly, or subjecting themselves to a physical and quite intrusive or aversive prompt.
Prompts are not a part of everyday life. Yes, you use them when you are in training, but after a few weeks, your boss expects you to take orders without even a verbal prompt. To get rid of prompts, you can either fade or delay the prompts. Prompt fading is when the prompt is gradually removed as it is no longer needed. Fading within a prompt means that you use just one prompt and once the person has the procedure down, you stop giving them a reminder or nudge. Maybe you are a quick study and the trainer only needs to demonstrate the correct procedure once (modeling). The trainer would simply discontinue use of the prompt. You can also use what is called fading across prompts. This is used when two or more prompts are needed. Maybe you are trying to explain an algebraic procedure to your child who is gifted in math. You could start with a verbal prompt and then move to gestural or modeling if they have a bit of an issue. Once the procedure is learned, you would not use any additional prompts. You are fading from least to most intrusive. But your other child is definitely not math oriented. In this case, modeling would likely be needed first and then you could drop down to gestural and verbal. This type of fading across prompts moves from most to least intrusive.
Finally, prompt delay can be used and is when you present the SD and then wait for the correct response to be made. You delay delivering any prompts to see if the person engages in the desirable behavior. If the person does, then no prompt is needed, but if not, then you use whichever prompt is appropriate at the time. For instance, you might tell your child to do the next problem and then wait to see if they can figure it out on their own. If not, you use the appropriate prompt.
6.6.2.3. Self-instructions. Earlier, I indicated that leaving cues for you to make the desired behavior is an effective antecedent manipulation. I have also said that self-instructions, or statements you write or say to yourself as positive affirmations and motivational tools, could be used too. These statements should remind yourself of what the desirable behavior is, why you are doing it (linked to your reason for change as discussed in Module 3), and what you hope to gain from it (your final goal). This may seem like a simple strategy and it is. It is low cost, low stakes, but very important. People use motivational statements all the time and even buy posters with their words printed across and hang them up. This is no different and you can hang these self-instructions of what to do around your house, in your car, have them on your phone, etc. If you are developing a self-modification plan, write them yourself and if you are working with a client on a behavior modification/ intervention plan, have them develop the statements. Then hang them up. Use them to replace self-defeating statements such as saying, “I am fat.” Instead, say, “I can lose the weight and be healthy.” When you need your statements, say them out loud. If you are having a moment of weakness in the grocery store (i.e. you forgot to go satiated), then use the statements to walk right by the junk food aisle.
6.6.2.4. Social support. Social support is a crucial strategy to implement in behavior modification. When executing a self-modification plan, we all will have moments of weakness and need reassurance from those closest to us. Or better yet, maybe we are doing really well and compliments and ‘likes’ on social media motivate us all the more. Social support has been shown to buffer against the negative effects of stress and when we make a public declaration of our goal, we are more likely to stick with it. In relation to the discussion at the end of Section 7.6, prompts require another person’s involvement in our plan and so go hand-in-hand with social support. Cues and self-instructions do not.
Be careful with social support though. It may be that the desired behavior we wish to make is being thwarted by tempting situations and people. In this case, you would likely not want to engage in social support, especially with the person bringing temptation into your plan. Maybe you want to stop eating Taco Bell late at night and do so because your roommate is always hungry late at night. This individual would likely not be a useful player in your behavior modification plan. Be aware of the effect other people have on your behaviors.
6.6.3. Behavior Focused Strategies
Now that we have covered procedures to use for controlling or manipulating the antecedent let’s move to what can be done about the behavior. This is really a set of unique procedures particular to special situations, such as creating a behavior that a person or animal would not normally know to do, reducing fear and anxiety, stopping bad habits, and replacing or removing unproductive thoughts. We will cover a few.
6.6.3.1. Shaping. Sometimes there is a new(ish) behavior we want a person or animal to make but they will not necessarily know to make it, or how to make it. As such, we need to find a way to mold this behavior into what we want it to be. The following example might sound familiar to you. Let’s say you want a friend to turn on the lights in the kitchen. You decide not to tell them this by voice but play a game with them. As they get closer to light switch you say “Hot.” If they turn away or do not proceed any further, you say “Cold.” Eventually, your statements of “Hot” will lead them to the switch and they will turn it on which will lead to delivery of a great big statement of congratulations. “Hot” and “Thank you” are reinforcers and you had them make approximations of the final, desired behavior of turning on the light. We called this ‘hot potato-cold-potato’ when we were a kid but in applied behavior analysis this procedure is called shaping by successive approximations or shaping for short. For shaping to work, the successive approximations must mimic the target behavior so that they can serve as steps toward this behavior.
6.6.3.2. Modifying fear and anxiety behaviors. To reduce or eliminate fear and anxiety, a few strategies can be used to include relaxation techniques and systematic and in-vivo desensitization. I will also mention a respondent conditioning technique called flooding and an observational learning strategy called modeling.
Maybe the simplest, and most important technique, is to just relax. Relaxation is designed to decrease ANS arousal that occurs with fear and anxiety. It comes in many forms and you are best to select the one you are most comfortable with. You must be able to use it quickly when fear and anxiety arise. Three common techniques include:
- Diaphragmatic breathing – Also called deep breathing; person breathes in a deep, slow rhythmic fashion. Many students use this technique right before giving an oral presentation.
- Progressive Muscle Relaxation or tension-release method – The person systematically tenses and relaxes each of the major muscle groups in the body and so they become more relaxed than in their initial state.
- Attention Focused Exercises – Relaxation occurs when attention is directed to a neutral or pleasant stimulus. This removes attention from the anxiety producing stimulus. It includes meditation, guided imagery, and hypnosis. Before giving that presentation, you might imagine being at home, safe in your room, in your bed, and under your covers. Or you might imagine anywhere else you would rather be such as at the beach or amusement park. Heck, you might even use the common strategy of imagining the audience in their underwear.
These techniques are easy to learn but must be practiced. Once learned, the new behavior, essentially an alternative behavior, will be used to replace the problem behavior of fear/anxiety. It is important to practice using it as often as possible so that the response generalizes across environments and situations. When needed, it will be easily available to you as a coping mechanism to avoid anxiety or fear. Essentially, it can become NR and is used as a type of avoidance behavior (taking away something aversive which is the fear and anxiety which makes the behavior of relaxing more likely in the future when we experience fear and anxiety). It is a good idea to pair relaxation techniques with self-instructions such that the latter serves as a reminder to do the former. But the self-instructions should be positive statements to help undue the ill effects of self-defeating statements. These techniques can be used with more than just fear and anxiety procedures too. You will find yourself selecting them as a strategy for a variety of target behaviors encountered in our exercises.
Relaxation techniques are important for the second major treatment strategy – desensitization. It may be classified as systematic in which the client imagines fear or anxiety producing scenarios or in-vivo in which the client experiences the fear/anxiety producing situations firsthand. To use systematic or in-vivo desensitization, you must learn at least one relaxation technique mentioned above. Once you do this, develop a fear hierarchy from the least fearful/anxiety producing to the most. Then, the client practices making the relaxation technique while the therapist has him or her imagine the scene from the hierarchy or experiences each situation. To help you remember what the two terms indicate, know that in-vivo is Latin for in life. Hence, in vivo is a real-life exposure while systematic is imagined.
Next, flooding is a respondent condition technique in which the person is exposed to the feared stimulus at full intensity for a prolonged period. If you have a fear of clowns, you would be thrown into a room of clowns in this method. Of course, initially, your anxiety would be greatly heightened. But over time, and with no negative events occurring, your anxiety would decrease through extinction. More on how this works in Module 10. In fact, this was the same example that was discussed with a better focus on respondent conditioning verbiage.
Finally, another non-operant conditioning procedure is to use what observational learning theorists call modeling. To help a person become less fearful or anxious, you could show them a video or live demonstration of a model approaching the feared stimulus or engaging in a fear-producing activity and having nothing bad happen to him or her. Upon seeing this, the client should feel more comfortable making the same behavior.
6.6.3.3. Habit behaviors. Dictionary.com defines a habit as “an acquired behavior pattern regularly followed until it has become almost involuntary” (http://www.dictionary.com/browse/habit). The habits do not harm anyone, other than possibly the person making them, but can be annoying for others if they increase in frequency, duration, and/or intensity. When this occurs, we are said to have a habit disorder. Habit behaviors take three main forms: nervous habits such as tapping one’s foot or twirling hair, tics (whether verbal or motor), and stuttering.
So how do we go about ending or reducing habit behaviors? Treatment includes the use of a habit reversal procedure with two main steps or components: awareness training and a competing or incompatible response.
To start, the client must be aware of exactly what the habit is, when it occurs, in what situations, and with whom around. A clear behavioral definition must be stated and explained to the client so that he or she can identify when the behavior is about to start or is occurring. This stage or step is called awareness training.
Next, a competing response must be identified that is incompatible with the habit and makes its occurrence nearly impossible or difficult. If you are trying to stop nail-biting, you can use a clenched fist, sitting on one’s hands, or holding a pencil as a competing response. You could even just groom your nails instead. If you have problems with motor tics, tense the affected body part and keep it still such as with head twitching. Tensing neck muscles and placing your chin against your chest will make head shaking or neck turning difficult to do. If you bite your lips, keep your lips and bottom teeth slightly separate. As a child, I stuttered and though today I do not daily, I find that there are certain trigger words that will elicit stuttering. Unfortunately, two of these trigger words are ones I at times use on a regular basis in classes – statistics and organizational (as in I/O psychology). Statistics is the main issue and to stop the stuttering before it starts, I will substitute statistics with stats, a one-syllable word and much easier to say or will pause in between saying the word such as ‘Sta’ and ‘tistics.” The pause is very brief and I do not make it noticeable. I then continue with my lecture as normal. This competing response allows me to say the word statistics in class and not endure any embarrassment from stuttering the word, which I have done in front of large lecture halls before. In terms of organizational, I usually just say I/O psychology and have the full word, with an acronym, on the slide being displayed. This way I can get away with the shorthand and if a student asks what it means, I just point to it on the slide.
The competing response should be made by the same body part involved in the nervous habit or tic and should be practiced in imagined situations. Imagine being in the situation that causes the habit, which you would have identified in your functional assessment, and rehearse making the competing response in your mind, called “mental practice.” This increases the likelihood of making the competing response when the habit occurs and so leads to generalization.
Now move to making the competing response in real life. Social support is key and significant others can offer the encouragement needed to make the competing response, deliver reinforcers once you made it, but maybe more importantly, they can utilize prompts to do so. Keep your reasons for making the behavior change in mind and utilize self-instructions as reminders when your motivation is low. Provide your own reinforcers to encourage making the competing response, and if they are something you really enjoy or are looking forward to, they can serve as establishing operations.
Finally, review how things went with your therapist. Remember, he or she cannot be with you 24/7 and so you need to talk about both your successes and failures and how they made you feel. If you were not able to make the competing response did the habit cause you embarrassment as stuttering or a tic might do, or just lead to frustration as any of the three might? Figure out if there are other antecedent triggers for the habit that might have been missed by the functional assessment. Then you can always practice making the competing response in these situations before doing it in real life.
6.6.3.4. Procedures for maladaptive cognitions. The final set of procedures focus specifically on what we think or feel, as part of the definition of behavior. The word cognition is used, which is the same as saying a thought. We will discuss several strategies that can be used to change these unwanted, maladaptive cognitions, whether they are present as an excess such as with paranoia, suicidal ideation, or feelings of worthlessness; or as a deficit such as with self-confidence and self-efficacy.
According to the National Alliance on Mental Illness (NAMI), cognitive behavioral therapy “focuses on exploring relationships among a person’s thoughts, feelings and behaviors. During CBT a therapist will actively work with a person to uncover unhealthy patterns of thought and how they may be causing self-destructive behaviors and beliefs.” CBT attempts to identifying negative or false beliefs and restructure them. They add, “Oftentimes someone being treated with CBT will have homework in between sessions where they practice replacing negative thoughts with more realistic thoughts based on prior experiences or record their negative thoughts in a journal.” For more on CBT, visit: https://www.nami.org/Learn-More/Treatment/Psychotherapy. Some commonly used strategies include cognitive restructuring, cognitive coping skills training, and acceptance techniques.
A second major strategy is to use what is called cognitive coping skills training. This strategy teaches social skills, communication, and assertiveness through direct instruction, role-playing, and modeling. For social skills, identify appropriate social behavior such as making eye contact, saying no to a request, or starting up a conversation with a stranger and whether the client is inhibited from making this behavior due to anxiety. For communication, determine if the problem is with speaking, listening, or both and then develop a plan for use in various interpersonal situations. Finally, assertiveness training aids the client to protect their rights and obtain what they want from others. Those who are not assertive are often overly passive and never get what they want or are overly aggressive and only get what they want. Treatment starts with determining situations in which assertiveness is lacking and coming up with a hierarchy of assertiveness opportunities. Least difficult situations are handled first, followed by more difficult situations, all while rehearsing and mastering all the situations present in the hierarchy. For more on these techniques, visit http://cogbtherapy.com/cognitive-behavioral-therapy-exercises/.
Finally, acceptance techniques can be used to reduce a client’s worry and anxiety. Life involves a degree of uncertainty and at times we need to just accept this. Techniques might include weighing the pros of fighting uncertainty against the cons of doing so. The cons should outweigh the pros and help you to end the struggle and accept what is unknown. Chances are you are already accepting the unknown in some areas of life and identifying these can help you to see why it is helpful in these areas, and how you can also think like this in more difficult areas. Finally, does uncertainty unnecessarily lead to a negative end? We may think so, but a review of the evidence for and against this statement will show that it does not and reduce how threatening it seems.
6.6.4. Consequence Focused Strategies
We now turn our attention to the last part of the ABCs of behavior, and specifically, the consequence. Our discussion will cover reinforcers, differential reinforcement, the token economy, self-praise, and punishment. We will also turn our attention back to social support and how it relates to the aforementioned strategies.
6.6.4.1. Differential reinforcement. Differential reinforcement is when we attempt to get rid of undesirable or problem behaviors by using the positive reinforcement of desirable behaviors. Hence, both reinforcement and extinction are occurring, the former in terms of the desired behavior and the latter in terms of the undesirable or problem behavior. Differential reinforcement does not utilize punishment but is a positive approach to reward people for behaving in the desired manner.
Differential reinforcement takes on many different forms as described below
- DRA or Differential Reinforcement of Alternative Behavior – This is when we reinforce the desired behavior and do not reinforce undesirable behavior. Hence, the desired behavior increases and the undesirable behavior decreases to the point of extinction. The main goal of DRA is to increase a desired behavior and extinguish an undesirable behavior such as a student who frequently talks out of turn. The teacher praises the child in front of the class when he raises his hand and waits to be called on and does not do anything if he talks out of turn. Though this may be a bit disruptive at first, if the functional assessment reveals that the reinforcer for talking out of turn is the attention the teacher gives, not responding to the child will take away his reinforcer. This strategy allows us to use the reinforcer for the problem behavior with the desirable behavior. Eventually, the child will stop talking out of turn making the problem behavior extinct.
- DRO or Differential Reinforcement of Other Behavior – What if we instead need to eliminate a problem behavior – i.e. reducing it down to no occurrences? DRO is the strategy when we deliver a reinforcer contingent on the absence of an undesirable behavior for some period. We will need to identify the reinforcer for the problem behavior and then pick one to use when this behavior does not occur. Determine how long the person must go without making the undesirable behavior and obtain a stopwatch to track the time. Do not reinforce the problem behavior and only reinforce the absence of it using whatever reinforcer was selected, and if it is gone for the full-time interval. If the problem behavior occurs during this time, the countdown resets. Eventually the person will stop making the undesirable behavior and when this occurs, increase the interval length so that the procedure can be removed. If a child squirms in his seat, the teacher might tell him if he sits still for 5 minutes he will receive praise and a star to put on the star chart to be cashed in at a later time (this is a token economy described in the next section). If he moves before the 5 minutes is up, he has to start over, but if he is doing well, then the interval will change to 10 minutes, then 20 minutes, then 30, then 45, and eventually 60 or more. At that point, the child is sitting still on his own and the behavior is not contingent on receiving the reinforcer. What I just described is how to use a DRO procedure and then how to get rid of it which will be critical in the maintenance phase.
- DRL or Differential Reinforcement of Low Rates of Responding – There are times when we don’t necessarily want to completely stop a behavior, or take it to extinction, but reduce the occurrence of a behavior. Maybe we are the type of person who really enjoys fast food and eat it daily. This is of course not healthy, but we also don’t want to go cold turkey on it. We could use DRL and decide on how many times each week we will allow ourselves to visit a fast food chain. Instead of 7 times we decide that 3 is okay. If we use full session DRL we might say we cannot exceed four times going to McDonalds in a week (defined as Mon – Sun). If we eat at McDonalds, Burger King, and/or Wendy’s, etc. four times on Monday but do not go again the rest of the week we are fine. Full session simply means you do not exceed the allowable number of behaviors during the specified time period. Eating fast-food four times in a day is definitely not healthy, and to be candid, gross, so a better approach could be to use spaced DRL. Now we say that we can go to a fast-food restaurant every other day. We could go on Monday, Wednesday, Friday, and Sunday. This works because we have not exceeded 4 behaviors in the specified time of one week.
- DRI or Differential Reinforcement of Incompatible Behavior – There are times when we need to substitute Behavior A with Behavior B such that by making B, we cannot make A. The point of DRI is to substitute a behavior. If a child is made to sit appropriately in his seat they cannot walk around the room. Sitting is incompatible with walking around. DRI delivers a reinforcer when another behavior is used instead of the problem behavior. To say it another way, we reinforce behaviors that make the undesirable or problem behavior impossible to make. DRI is effective with habit behaviors such as thumb sucking. We reinforce the child keeping his hands in his pocket. Or what if a man tends to make disparaging remarks at drivers who cut him off or are driving too slowly (by his standard)? This might be a bad model for his kids and so the man’s wife tells him to instead say something nice about the weather or hum a pleasant tune when he becomes frustrated with his fellow commuters. These alternative behaviors are incompatible with cursing and she rewards him with a kiss when he uses them.
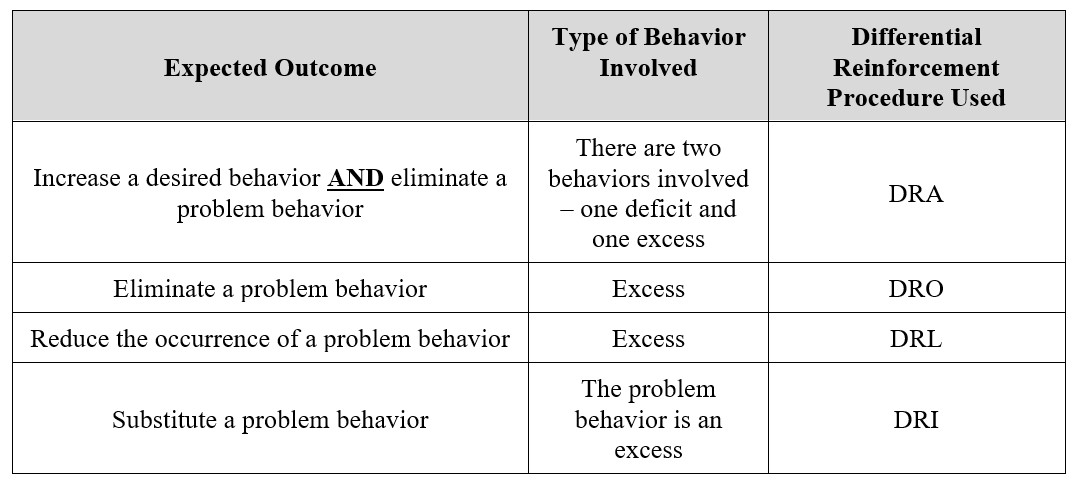
It is important to keep in mind the following:
Table 6.3: Expected Outcome and Type of Differential Reinforcement to Use
6.6.4.2. Token economy. A token economy is a fun system that allows the person to earn up tokens and then cash them in for some type of reinforcer — whether a consumable, activity, privilege, or tangible. The tokens are accrued (and accumulated over time) once the target behavior occurs, as described clearly in the behavioral definition, and by themselves have no meaning. That said, it is fine to praise the person as they receive their tokens (a second PR, the first being the receipt of the tokens). Be clear on how many tokens are earned for engaging in the desired behavior(s).
Tokens gain meaning when they are associated with backup reinforcers or the regular reinforcers the person has in their life. This association occurs because the individual learns that he or she can take some number of tokens and cash them in for some amount of reinforcer. When we go to the store to purchase milk, we read the label and see that the gallon costs $3.29. We pick it up, go to the cashier, and when prompted, hand the cashier our money to complete the purchase. The token economy operates in the same exact fashion. How many tokens are needed to purchase a backup reinforcer is called the exchange rate. What can serve as a token? Bingo chips, stars on a chart, points, check marks, or poker chips can all be used, and it must be clear how many tokens are earned for engaging in a certain level of the behavior.
The token economy can be used at home by parents trying to get a child to complete chores, take a bath before playing video games, eat breakfast, behave well with siblings, or leave with enough time to get the bus or arrive at school before the bell rings. In the classroom, a teacher can use a token economy to encourage students to study hard, stay in their seat during quiet time, put away class materials, talk with an inside voice, behave on the playground, throw away their trash at lunchtime, or to walk and not run through the halls. At work, an employer may wish to reward employees for working safely, going above and beyond by serving on committees, being on time, exceeding performance standards, or positively approaching all aspects of their job. In a recovery center, nursing home, or prison setting, tokens may be awarded when patients take their medications or are compliant with the direction of staff members.
6.6.4.3. Punishment. Punishment is an aversive consequence meant to deter an unwanted behavior. Probably the most well-known of all punishment procedures is the time out. Simply, a time out is when a person is removed from an activity because they are engaging in an undesirable or problem behavior. If effective, the time out should result in a reduction of the problem behavior in the future and so functions as a negative punishment (NP; taking away something good (the fun activity which serves as a reinforcement) making a behavior less likely in the future).
Time outs take two forms – exclusionary or non-exclusionary. Exclusionary time outs are when the person is removed from the actual location where the problem behavior is occurring. The best example, and the one you might be thinking of, is when a teacher sends a child to the principal’s office. Obviously then, a child is not removed from the situation in a non-exclusionary time out but cannot partake in the reinforcing activity. Depending on what the activity is, I might say that non-exclusionary is more punishing. Why is that? If a child misbehaves on the playground and the teacher makes him sit on the side, he still can see all the fun the other kids are having but cannot participate. This is worse than being sent inside to sit at a table or talk with the principal, and not being able to see and hear all the fun that is going on.
6.6.4.4. Response cost. Simply, a response cost is a type of negative punisher in which some amount of a reinforcer is removed when a problem/undesirable behavior is engaged in.
6.6.4.5. Overcorrection procedures. Did you ever throw a tantrum and trash your room? Have you become so upset at someone that you yelled at them for a period of time? If so, you engaged in a problem behavior and likely were punished for doing so. If in the context of your childhood home, your parents may have made you clean your room up and make it look better than it did before, or be extra nice to your sibling. These are types of overcorrection procedures or when a person is expected to engage in effortful behavior for an extended period after the occurrence of an undesirable behavior. The example of cleaning the room is called restitution, or restoring the environment to a condition that is better than it was before the undesirable behavior, and being super nice is called positive practice, or engaging in the correct form of behavior over and over again.
******************************************************************************
Note to Student: Be advised that before implementing our plan, we need to also need to identify mistakes. Mistakes are just what they sound like — errors we make in designing or implementing our plan.
We also need to establish rules. Rules are statements that add order, predictability, and reliability to our plan and can take the If-Then format. At the same time, we will develop a behavioral contract or a written agreement between two people in which at least one of the two has agreed to engage in a specific level of the target behavior.
Covering these topics is beyond the point of this module. See the Principles of Behavior Analysis and Modification (Daffin, 2021) textbook for more information on these topics. The full text can be accessed by clicking here.
******************************************************************************
6.7. Implementing the Plan
Section Learning Objectives
- Define the treatment phase.
Now that you have a behavior modification plan to change your target behavior for the good, it is time to implement the plan and see how it works. The treatment phase is when you employ all antecedent, behavior, and consequence-focused strategies. In the grand scheme of scientific research and specifically experiments, the treatment phase, but more so the strategies, are your IV or independent variable. Remember, this is the one that is manipulated. You have chosen certain strategies and decided to use them in a specific way which is the essence of manipulation. No matter what, manipulation is at work but so is measurement. Behavior is measured via your goals and behavior counts and is the dependent variable or DV.
6.8. Evaluating the Plan’s Success
Section Learning Objectives
- Clarify what to do if you have to change your target behavior.
As you are going through your plan it is a good idea to see how you are doing. Fortunately, you are collecting a great deal of data and so have all you need to make a determination.
If you need to adjust your plan, you need to figure out what is making your plan difficult to achieve. Likely, you will have at least one issue with your antecedents, behavior, and/or consequences. Look closely at the data you gathered and your notes in the journal which you keep with the ABC chart during the treatment phase. It might be that you set unrealistic goals, had a faulty criterion for when to move from one goal to the next, had issues with how to record your data, your strategies may not have worked, there were temptations in your environment you were not aware of, or your social support really was not supportive. Of course, there can be countless other issues that you may encounter.
Once you have figured out needed changes to your plan, implement them. Continue the process of evaluation and adjustment until your plan works or you just cannot seem to reduce the unwanted behavior or increase a desirable one.
Assuming your plan works, and the behavior has changed in the hypothesized manner, you will proceed to the maintenance phase.
6.9. Maintenance Phase and Relapse Prevention
Section Learning Objectives
- Describe the function of the maintenance phase.
- Differentiate a lapse and a relapse.
6.9.1. Maintenance Phase
When planning to change our behavior we cannot lose sight of the fact that eventually, we will obtain our final goal. At this point, the target behavior is now occurring habitually or without conscious effort, or due to the use of the many strategies we selected. Once this occurs, we need to transition from the treatment phase to the maintenance phase. The strategies used during the treatment phase cannot remain in effect for the duration of our life, so we must phase them out…well, most of them. Some strategies you will want to keep in place. Outside of noting that, a more exhaustive discussion is beyond the scope of this book.
As with all things in life, we hit bumps in the road. We hit them when planning our behavior modification plan, likely hit a few as we employed the treatment, and even in the maintenance phase, we may hit some. In fact, there are two types of issues we may encounter during the maintenance phase:
- Maintenance Problem — Though we have gone to great lengths to ensure our target behavior stays at our desired level, based on the final goal, at times we falter. This is not necessarily due to a return to a problem or undesirable behavior, but maybe just a loss of motivation for walking your dog every night, reading at bedtime, going to the gym, drinking water, studying more regularly, etc.
- Transfer Problem — Recall that we want to generalize our new behavior beyond just training situations/environments. If we establish good study habits when in our dorm, we want to do the same when studying in the student union or in the library. If we go to the gym regularly while at school, we want to do so at home on break. Or maybe you are studying well in all places, but this positive behavior only occurs for classes in your major. In all other classes, your poor study habits have not changed. So, you are performing as well as you want to in some instances, but not in all instances. The desirable behavior has not transferred or generalized as expected.
6.9.2. Relapse Prevention
Before understanding how to prevent relapse, we have to distinguish the terms lapse and relapse. Simply, a lapse is when we make a mistake or slip up. Consider the expression, “Having a lapse in judgment.” This implies that we generally make sound decisions but in this one instance we did not. We made a mistake. What we do not want is an isolated incident becoming a pattern of behavior. When this occurs, we have a relapse. Do not beat yourself up if a lapse occurs. Our problem behavior will inevitably return at some point. We just do not want it sticking around for the long term.
There are people and things that tempt us and situations or places that lead us to temptation more than others. To avoid a lapse turning into a relapse, take special note of high-risk situations and environments, and the people who are present when we cave into temptation. Keeping good records of the ABCs of behavior, and your journal, will help you to identify these situations and people. Then you can develop new plans to deal with them or to re-establish old ones.
For more information on relapse and how to prevent it, see Module 14 of the behavior modification textbook.
Module Recap
In Module 6, we discussed a willingness to change from the perspective of DiClimente’s process of change. We also discussed self-efficacy and how believing in ourselves will make success more likely. Of course, success is never guaranteed, and everyone makes mistakes or gives in to temptation. These lost battles do not mean the war is lost though.
We then discussed the need to precisely define our target and competing behaviors. Once a precise definition is in place, we can formulate goals for how much we wish for the behavior to increase or decrease. We can also set short term or proximal goals to help us achieve the much larger or distal goal. Think about writing a 10-page paper. It is easier to say I am going to write the first section today, the next tomorrow, and then the final section the day after. Then I will revise and edit and print the paper to be submitted. These subgoals make the much larger task more manageable and easier to achieve. As this works with writing a paper, so too it can work with changing behavior.
Next, we discussed ways to collect data about the behavior, what causes it, and what maintains it. The baseline phase is when we record occurrences of the behavior before any manipulation/strategies are employed. From this we conduct a functional assessment and discussed what information we can gain from it. We also had a discussion of temptations and what to do about them.
We discussed the strategies used to change an unwanted behavior or to establish a new behavior. These focused on the antecedent and included goal setting, antecedent manipulations, prompting and fading, self-instructions, and social support. Then we discussed the behavior focused strategies of shaping, fear and anxiety procedures, habit reversal, and cognitive behavior modification. We finished up by discussing consequence focused strategies focusing on the use of reinforcement and punishment.
As we winded down Module 6, we discussed the important issue of evaluating the plan and making adjustments as needed. Finally, we discussed the final stage of our behavior modification plan — maintenance. Knowing when to move to this stage is half the battle and the other half is knowing what to do when we have maintenance or transfer issues. Our bad behavior will rear its ugly head, and this is to be expected, but what we need to do is prevent it from becoming the norm and not the exception. This is where relapse prevention comes in. Effective stress management can go a long way to helping us to avoid tempting people, things, situations, and environments, and to allow rational processes to govern our behavior.
Is there a behavior you want to decrease (an excess) or increase, either from a complete non-occurrence or minimal occurrence now (deficit)? If so, are you motivated to bring about such change? Whether you are or not, hopefully this module gave you some things to think about and a foundation to start your planning process. Please visit the Principles of Behavior Analysis and Modification if you are serious about this journey.
2nd edition
